Tải xuống bản thuyết trình
Bản thuyết trình đang được tải. Xin vui lòng chờ

1
CẬP NHẬT COPD VÀ VAI TRÒ THUỐC GIÃN PQ TRONG ĐIỀU TRỊ
Pgs ts bs trần văn ngọc

2
COPD thay đổi thứ tự nguyên nhân gây tử vong trên thang đánh giá
Đến năm 2030, COPD được dự đoán là nguyên nhân thứ 3 gây tử vong trên toàn cầu 2015 2030 Rank Cause of Death % Cause of Deaths 1 Ischaemic heart disease 13.2 2 Stroke 11.7 12.2 3 Lower respiratory infections 5.6 COPD 6.5 4 5.0 5 Diarrhoeal diseases 3.2 Diabetes mellitus 3.5 6 HIV/AIDS 2.9 Trachea, bronchus, lung cancers 3.4 7 Road injury 2.6 8 2.7 9 2.5 2.3 10 Hypertensive heart disease 2.0 2.1

3
Đợt kịch phát nhập viện liên quan đến tăng tỷ lệ tử vong
Kaplan-Meier plot showing risk of mortality in patients with COPD with and without hospitalized exacerbations during the first 12 months of follow-up Hosp, hospitalization Schmidt SA, et al. BMJ Open 2014; 4: e006720; Mullerova H, et al. Chest 2015; 147: 999–1007.

4
COPD là gánh nặng toàn cầu
> 380 triệu BN COPD Nguyên nhân tử vong thứ 5 Tăng tần suất Chẩn đoán và điều trị dưới mức thực tế

5
30% of cigarettes consumed in China
Top 10 hút thuốc lá Indonesia: 4thlargest cigarette consumers in the world 30% of cigarettes consumed in China Key Point Worldwide, 1.25 billion people are smokers. Although the overall prevalence in men is declining slowly, smoking prevalence in women is increasing in some countries. Background Worldwide, smoking is highly prevalent at 1.25 billion people, with marked differences in prevalence patterns and trends between men and women.1 For example, in the US and Canada, smoking prevalence is approximately the same in both men and women at 20%–29% (23%, US; 20%–30%, Canada).1-3 In contrast, in Italy, Australia, and Spain, prevalence is lower in women. In developed countries, 35% of men and 22% of women smoke. In contrast, in developing countries, although 50% of men smoke, only 9% of women are smokers. Overall, in men, the prevalence of smoking is declining. However, in women, although smoking prevalence is declining in some countries, such as the United States, the United Kingdom, Australia, and Canada, in several southern, central, and eastern European countries, smoking prevalence is not in decline or is still increasing.1 References 1. Mackay J, Eriksen M. The Tobacco Atlas. Geneva, Switzerland: World Health Organization; 2002. 2. Giovino GA. Epidemiology of tobacco use in the United States. Oncogene. 2002;21:7326–7340. 3. Lemiere C, Boulet LP. Cigarette smoking and asthma: a dangerous mix. Can Respir J. 2005;12:79–80. Eriksen M. Mackay J The Tobacco Atlas. World Health Organization. 2015;
6
Tần suất nam/nữ hút thuốc lá 2008-13
Male Key Point Worldwide, 1.25 billion people are smokers. Although the overall prevalence in men is declining slowly, smoking prevalence in women is increasing in some countries. Background Worldwide, smoking is highly prevalent at 1.25 billion people, with marked differences in prevalence patterns and trends between men and women.1 For example, in the US and Canada, smoking prevalence is approximately the same in both men and women at 20%–29% (23%, US; 20%–30%, Canada).1-3 In contrast, in Italy, Australia, and Spain, prevalence is lower in women. In developed countries, 35% of men and 22% of women smoke. In contrast, in developing countries, although 50% of men smoke, only 9% of women are smokers. Overall, in men, the prevalence of smoking is declining. However, in women, although smoking prevalence is declining in some countries, such as the United States, the United Kingdom, Australia, and Canada, in several southern, central, and eastern European countries, smoking prevalence is not in decline or is still increasing.1 References 1. Mackay J, Eriksen M. The Tobacco Atlas. Geneva, Switzerland: World Health Organization; 2002. 2. Giovino GA. Epidemiology of tobacco use in the United States. Oncogene. 2002;21:7326–7340. 3. Lemiere C, Boulet LP. Cigarette smoking and asthma: a dangerous mix. Can Respir J. 2005;12:79–80. Female
.1-3 In contrast, in Italy, Australia, and Spain, prevalence is lower in women. In developed countries, 35% of men and 22% of women smoke. In contrast, in developing countries, although 50% of men smoke, only 9% of women are smokers. Overall, in men, the prevalence of smoking is declining. However, in women, although smoking prevalence is declining in some countries, such as the United States, the United Kingdom, Australia, and Canada, in several southern, central, and eastern European countries, smoking prevalence is not in decline or is still increasing.1. References. 1. Mackay J, Eriksen M. The Tobacco Atlas. Geneva, Switzerland: World Health Organization; Giovino GA. Epidemiology of tobacco use in the United States. Oncogene. 2002;21:7326– Lemiere C, Boulet LP. Cigarette smoking and asthma: a dangerous mix. Can Respir J. 2005;12:79–80. Female.")
7
COPD không hút thuốc : chất đốt sinh khối
% dân số tiếp xúc với chất đốt sinh khối

8
Bệnh nhân COPD thường được chẩn đoán khi đã ở giai đoạn nặng
GOLD % GOLD 4 5% GOLD % At diagnosis, 50% of COPD patients are already suffering from moderate disease (GOLD 2). Data collected from medical charts and administrative claims in a managed care data repository. GOLD % Patients typically present at GOLD 2 (moderate disease). BN thường ở giai đoạn GOLD 2 (mức độ trung bình) khi được chẩn đoán. Nhiều bệnh nhân thường chưa được chẩn đoán bệnh cho đến khi tắc nghẽn nặng. Mapel DW, et al. Int J Chron Obstruct Pulmon Dis 2011; 6: 573–581.
. Data collected from medical charts and administrative claims in a managed care data repository. GOLD 3 26% Patients typically present at GOLD 2 (moderate disease). BN thường ở giai đoạn GOLD 2 (mức độ trung bình) khi được chẩn đoán. Nhiều bệnh nhân thường chưa được chẩn đoán bệnh cho đến khi tắc nghẽn nặng. Mapel DW, et al. Int J Chron Obstruct Pulmon Dis 2011; 6: 573–581.")
9
QUẢN LÝ VÀ ĐIỀU TRỊ COPD Xây dựng mô hình quản lý và điều trị
Cung ứng đủ thuốc BHYT chi trả Kiểm tra sự tuân thủ điều trị của BN Kiểm soát tốt đợt cấp Quản lý các bệnh đồng mắc

10
MÔ HÌNH QUẢN LÝ

11
Điều trị COPD ổn định • GOLD 2016 • GOLD 2017
Điều trị bằng thuốc cho COPD giai đoạn ổn định cho các nhóm BN GOLD ABCD cũng như nâng bậc hay hạ bậc điều trị là tùy theo đánh giá của từng cá thể về triệu chứng và nguy cơ cơn cấp • GOLD 2016 • GOLD 2017 Patient Group Recommended First Choice Alternative Choice Other Possible Treatments A SAMA or SABA LAMA or LABA or SABA and SAMA Theophylline B LAMA and LABA SABA and/or SAMA C ICS + LABA or LAMA LAMA and PD-4 inhibitor or LABA and PD-4 inhibitor SABA and/or SABA D and/or LAMA ICS + LABA and LAMA ICS + LABA and PD-4 inhibitor or LAMA and PD-4 inhibitor Carbocysteine N-acetylcysteine Group C Group D LAMA + LABA LABA + ICS Consider roflumilast* Consider macrolide** Vẫn còn cơn cấp) Vẫn còn cơn cấp LAMA + LABA + ICS Persistent symptoms /further Further exacerbation(s) exacerbation(s) LAMA LAMA + LABA LABA + ICS LAMA Group A Group B Continue, stop or try alternative class of bronchodilator LAMA + LABA evaluate effect Triệu chứng dai dẳng A bronchodilator A LABD (LABA or LAMA) Preferred treatment *xem xét đối với BN có FEV1 < 50% so với dự đoán và viêm PQ mạn ** trên người từng hút thuốc CAT, COPD Assessment Test; COPD, Chronic Obstructive Pulmonary Disease; FEV1, forced expiratory volume in 1 second; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroid; LABA, long-acting beta2-agonist; LAMA, long-acting
 Vẫn còn cơn cấp. LAMA + LABA + ICS. Persistent symptoms. /further. Further exacerbation(s) exacerbation(s) LAMA. LAMA + LABA. LABA. + ICS. LAMA. Group A. Group B. Continue, stop or try alternative class of bronchodilator. LAMA + LABA. evaluate effect. Triệu chứng dai dẳng. A bronchodilator A LABD (LABA or LAMA) Preferred treatment. *xem xét đối với BN có FEV1 < 50% so với dự đoán và viêm PQ mạn. ** trên người từng hút thuốc. CAT, COPD Assessment Test; COPD, Chronic Obstructive Pulmonary Disease; FEV1, forced expiratory volume in 1 second; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICS, inhaled corticosteroid; LABA, long-acting beta2-agonist; LAMA, long-acting.")
12
COPD TUÂN TRỊ KÉM Tỷ lệ tuân trị kém trong COPD là rất phổ biến:
49,4% dưới mức, > 50% quá mức (có triệu chứng) 31% dùng sai kỹ thuật bình xịt, hút Tỷ lệ tuân trị kém thay đổi tùy theo: Loại thuốc và chế độ liều dùng Công cụ theo dõi dùng thuốc: bộ đếm liều Đặc tính riêng biệt của từng cá nhân Bryant et al. Respiratory Research 2013, 14:109
 31% dùng sai kỹ thuật bình xịt, hút. Tỷ lệ tuân trị kém thay đổi tùy theo: Loại thuốc và chế độ liều dùng. Công cụ theo dõi dùng thuốc: bộ đếm liều. Đặc tính riêng biệt của từng cá nhân. Bryant et al. Respiratory Research 2013, 14:109.")
13
CÁCH CẢI THIỆN TUÂN TRỊ Tư vấn tầm quan trọng của việc tuân thủ điều trị Theo dõi tuân thủ sử dụng thuốc và ý kiến BN Cung cấp bảng kế hoạch hành động, giáo dục sức khỏe. Bryant et al. Respiratory Research 2013, 14:109

14
CÂU LẠC BỘ BN HEN VÀ COPD BV PHỔI TW “ GIỮ CHO LÁ PHỔI KHỎE MẠNH”
1. Về tổ chức: Giám đốc BV quyết định thành lập, có BCN, tư vấn viên được đào tạo về Hen,COPD, kĩ năng tư vấn. Mục tiêu: Tư vấn thường xuyên - giúp hội viên trở thành “thầy thuốc của chính mình” . Thành phần; Bệnh nhân, người nhà, tình nguyện 2. Tổng số cấp thẻ: 5000 hội viên. Tổng số lượt hội viên: 6.000 Sinh hoạt: Lịch cố định 9h sáng thứ bảy tuần đầu tiên của tháng tại Ht Hành chính BV Nội dung: 12 nội dung cơ bản trong quản lý Hen/COPD Hình thức: Bài giảng, thảo luận,thực hành mẫu, giải đáp. Báo cáo viên: BCN, bác sĩ, tư vấn viên và HV giàu kinh nghiệm.

15
Bệnh sử tự nhiên của đợt cấp COPD nặng
Suissa et al Thorax 2012 in Press Suissa S et al., Thorax Nov;67(11):957-63
:")
16
OUTCOME OF COPD EXACERBATIONS
Hospital mortality 20%-24% (1 year) In ICU patients In hospitalized patients Hospital mortality 2.5%-10% (5 days) TỬ VONG BN AECOPD NHẬP VIỆN BVCR 2010 : 10% , ĐẶT NKQ THỞ MÁY : 50% Treatment failure is defined as not responsive to initial treatment(s). Outcomes = health utilizations. This slide shows outcomes of patients with acute exacerbations: 20-24% of patients in the ICU with an exacerbation died; 6-12% of patients in general hospital beds, not ICU beds, died. Of those who visited the ER for an acute exacerbation, 22-32% of those patients had to revisit the emergency room after being discharged. Those who were treated as outpatients 13-33% of those patients did not response to initial treatments and needed further medical intervention. Main point: Acute exacerbations are a serious matter and should be of concern to the health care provider. Relapse (repeat ER visit) 22%-32% (14 days) In ER patients 13%-33% (14 days) Treatment failure rate In outpatients Seneff MG, Wagner DP, Wagner RP, Zimmerman JE, Knaus WA. Hospital and 1-year survival of patients admitted to intensive care units with acute exacerbation of chronic obstructive pulmonary disease. JAMA. 1995;274: Murata GH, Gorby MS, Chick TW, Halperin AK. Treatment of decompensated chronic obstructive pulmonary disease in the emergency department—correlation between clinical features and prognosis. Ann Emerg Med. 1991;20: Adams SG, Melo J, Luther M, Anzueto A. Antibiotics are associated with lower relapse rates in outpatients with acute exacerbations of COPD. Chest. 2000;117: Patil SP, Krishnan JA, Lechtzin N, Diette GB. In-hospital mortality following acute exacerbations of chronic obstructive pulmonary disease. Arch Int Med. 2003; 160: Seneff et al. JAMA. 1995; 274: ; Murata et al. Ann Emerg Med. 1991;20: ; Adams et al. Chest. 2000; 117: ; Patil et al. Arch Int Med. 2003; 163:
 In ICU patients. In hospitalized. patients. Hospital mortality. 2.5%-10% (5 days) TỬ VONG BN AECOPD NHẬP VIỆN BVCR 2010 : 10% , ĐẶT NKQ THỞ MÁY : 50% Treatment failure is defined as not responsive to initial treatment(s). Outcomes = health utilizations. This slide shows outcomes of patients with acute exacerbations: 20-24% of patients in the ICU with an exacerbation died; 6-12% of patients in general hospital beds, not ICU beds, died. Of those who visited the ER for an acute exacerbation, 22-32% of those patients had to revisit the emergency room after being discharged. Those who were treated as outpatients 13-33% of those patients did not response to initial treatments and needed further medical intervention. Main point: Acute exacerbations are a serious matter and should be of concern to the health care provider. Relapse (repeat ER visit) 22%-32% (14 days) In ER patients. 13%-33% (14 days) Treatment failure rate. In outpatients. Seneff MG, Wagner DP, Wagner RP, Zimmerman JE, Knaus WA. Hospital and 1-year survival of patients admitted to intensive care units with acute exacerbation of chronic obstructive pulmonary disease. JAMA. 1995;274: Murata GH, Gorby MS, Chick TW, Halperin AK. Treatment of decompensated chronic obstructive pulmonary disease in the emergency department—correlation between clinical features and prognosis. Ann Emerg Med. 1991;20: Adams SG, Melo J, Luther M, Anzueto A. Antibiotics are associated with lower relapse rates in outpatients with acute exacerbations of COPD. Chest. 2000;117: Patil SP, Krishnan JA, Lechtzin N, Diette GB. In-hospital mortality following acute exacerbations of chronic obstructive pulmonary disease. Arch Int Med. 2003; 160: Seneff et al. JAMA. 1995; 274: ; Murata et al. Ann Emerg Med. 1991;20: ; Adams et al. Chest. 2000; 117: ; Patil et al. Arch Int Med. 2003; 163:")
17
TÓM TẮT YẾU TỐ TIÊN LƯỢNG KIỂU HÌNH COPD ĐỢT CẤP THƯỜNG XUYÊN
Tuổi cao COPD nền tảng: Khó thở nhiều; FEV1 thấp; PaO2 thấp Tiền căn có đợt cấp thường xuyên Viêm đường thở hay toàn thân nhiều Vi khuẩn thường trú cao trong giai đoạn ổn định Kiểu hình viêm phế quản mạn tăng tiết đàm nhiều Bệnh đồng mắc trong và ngoài phổi: bệnh tim mạch, trầm cảm lo âu, bệnh cơ, trào ngược dạ dày thực quản 1 Marc Miravitlles et al (2012), Arch Bronconeumol, 48(3):86–98
, Arch Bronconeumol, 48(3):86–98.")
18
COPD CÓ ĐỢT CẤP THƯỜNG XUYÊN
GOLD 2013 – 2015 : đợt cấp thường xuyên : ≥ 2 đợt cấp/ năm HOẶC ≥ 1 đợt cấp phải nhập viện / năm Tuy nhiên các đợt cấp này cần cách nhau 1 ≥ 4 tuần sau khi ngưng điều trị đợt cấp cũ HOẶC ≥ 6 tuần kể từ khởi phát đợt cấp cũ nếu để tự nhiên Hai thời gian mốc này dùng để phân biệt giữa đợt cấp mới và thất bại điều trị đợt cấp cũ 1 Marc Miravitlles et al (2012), Arch Bronconeumol, 48(3):86–98
, Arch Bronconeumol, 48(3):86–98.")
19
YẾU TỐ TIÊN LƯỢNG COPD ĐỢT CẤP THƯỜNG XUYÊN
N/c Emily S Wan trên BN COPD nặng 1 FEF 25%–75% thấp: OR = 0,53 [0,28 – 0.98] mMRC cao: OR = 1,50 [1,15 – 1,97] Hen chẩn đoán trước đây: OR = 2,05 [1,16 – 3,64] N/c Y-M. Oh trên BN COPD mọi mức độ 2 Chỉ số khí phế thủng cao / CT scan định lượng RV/TLC cao qua đo phế thân ký Protein huyết tương thấp 1 Emily S. Wan et al. Respiratory Medicine (2011); 105, 588 – 594 2 Y–M. Oh et al. Int J Turberc Lung Dis (2014); 18 (12):1407–1414
; 105, 588 – Y–M. Oh et al. Int J Turberc Lung Dis (2014); 18 (12):1407–1414.")
20
Các yếu tố nguy cơ khiến bệnh nhân với đợt cấp COPD phải nhập viện
Nhập viện và tái nhập viện vì đợt cấp COPD có tương quan với các yếu tố sau: Hút thuốc liên tục Tăng PaCO2 FEV1 thấp tại thời điểm xuất hiện đợt cấp Có sử dụng corticoid (uống và xịt) Chỉ số BMI thấp Có tiền sử nhập viện. Chẩn đoán COPD trên 5 năm Có bệnh kèm theo (tim mạch, tiểu đường) Tuổi cao Sức khoẻ chung không tốt Khó thở nhiều Bahadori và cộng sự thực hiện một phân tích hệ thống để xác định các yếu tố nguy cơ nhập viện hoặc tái nhập viện do đợt cấp COPD. Phân tích này cung cấp bằng chứng cho các chính sách y tế quan trọng. Trong số các yếu tố được phân tích, chỉ số PaCO2 tăng là một thông số được báo cáo ở nhiều nghiên cứu nhất (52%) là một yếu tố nguy cơ nhập viện. Tương tự như vậy, FEV1 thấp và sử dụng corticoid liều cao (uống hoặc hít) cũng có liên quan với nguy cơ tái nhập viện vì đợt cấp COPD cao hơn. Sức khoẻ thể chất thấp có liên quan đến nhập viện vì COPD và nguy cơ phải cần người chăm sóc, mặc dù không thực sự rõ ràng. Cả thuốc hút thuốc lá chủ động và thụ động đều được xác định là các yếu tố nguy cơ nhập viện (P<0.0001). Bahadori K et al. Int J Chron Obstruct Pulmon Dis 2007; 2: 241–251 Bahadori K et al. Int J Chron Obstruct Pulmon Dis 2007; 2: 241–251
 Chỉ số BMI thấp. Có tiền sử nhập viện. Chẩn đoán COPD trên 5 năm. Có bệnh kèm theo (tim mạch, tiểu đường) Tuổi cao. Sức khoẻ chung không tốt. Khó thở nhiều. Bahadori và cộng sự thực hiện một phân tích hệ thống để xác định các yếu tố nguy cơ nhập viện hoặc tái nhập viện do đợt cấp COPD. Phân tích này cung cấp bằng chứng cho các chính sách y tế quan trọng. Trong số các yếu tố được phân tích, chỉ số PaCO2 tăng là một thông số được báo cáo ở nhiều nghiên cứu nhất (52%) là một yếu tố nguy cơ nhập viện. Tương tự như vậy, FEV1 thấp và sử dụng corticoid liều cao (uống hoặc hít) cũng có liên quan với nguy cơ tái nhập viện vì đợt cấp COPD cao hơn. Sức khoẻ thể chất thấp có liên quan đến nhập viện vì COPD và nguy cơ phải cần người chăm sóc, mặc dù không thực sự rõ ràng. Cả thuốc hút thuốc lá chủ động và thụ động đều được xác định là các yếu tố nguy cơ nhập viện (P<0.0001). Bahadori K et al. Int J Chron Obstruct Pulmon Dis 2007; 2: 241–251. Bahadori K et al. Int J Chron Obstruct Pulmon Dis 2007; 2: 241–251.")
21
Các đợt cấp COPD có liên quan đến tình trạng bệnh tiến triển
Các đợt cấp làm bệnh COPD nặng lên và tăng tỷ lệ tử vong. Các đợt cấp thường xuyên làm tăng chi phí y tế và ảnh hưởng đến chất lượng sống. Các đợt cấp làm chức năng hô hấp suy giảm nhanh hơn. “Một đợt cấp của COPD được định nghĩa là tình trạng nặng lên nhanh chóng của các triệu chứng hô hấp, vượt trên mức dao động của triệu chứng hàng ngày và đòi hỏi thay đổi thuốc” [1]. Các đợt cấp là một phần trong diễn tiến tự nhiên của COPD, với tần xuất tăng từ 1-4 lần mỗi năm ở những trường hợp COPD nặng. Có khoảng 3-16% các đợt cấp của COPD cần phải nhập viện, và tỷ lệ tử vong của các đợt cấp trầm trọng có thể lên đến 10% [2]. Số liệu từ các nghiên cứu đã cho thấy mức độ suy giảm chức năng phổi có liên quan đến số các đợt cấp xuất hiện [3] và, cũng không ngạc nhiên lắm, rằng các đợt cấp làm giảm chất lượng sống của bệnh nhân [4]. Các nghiên cứu cũng cho thấy các chiến lược quản lý và dự phòng bệnh tốt có thể ngăn ngừa các đợt cấp, ảnh hưởng tích cực đến tình trạng người bệnh và giảm chi phí y tế Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines Available from: Celli BR et al. Eur Respir J 2004; 23: 932–946 McIvor A et al. Can Fam Phys 2009; 55: 15–16 Donaldson CG et al. Thorax 2002; 57: 847–52 GOLD guidelines, Available from: Celli BR et al. Eur Respir J 2004; 23: 932–946 McIvor A et al. Can Fam Phys 2009; 55: 15–16
 guidelines Available from: Celli BR et al. Eur Respir J 2004; 23: 932–946. McIvor A et al. Can Fam Phys 2009; 55: 15–16. Donaldson CG et al. Thorax 2002; 57: 847–52. GOLD guidelines, Available from: Celli BR et al. Eur Respir J 2004; 23: 932–946. McIvor A et al. Can Fam Phys 2009; 55: 15–16.")
22
LIÊN QUAN ĐỢT CẤP COPD VÀ BỆNH ĐỒNG MẮC
Đợt cấp COPD bệnh đồng mắc nặng thêm NMCT ↑ 2,27 lần 5 ngày từ lúc khởi phát đợt cấp Loãng xương & suy dinh dưỡng ↑ do ↓ năng lượng Bệnh đồng mắc đợt cấp COPD nhiều thêm Suy tim, thuyên tắc phổi là nguyên nhân chính tử vong sớm trong COPD đợt cấp ↑ đường huyết ↑ thời gian nằm viện & tử vong Trầm cảm, lo âu ↑ tái phát, ↑ thời gian nằm viện Comorbidities of COPD. Eur Respir Rev 2013; 22: 454 – 475

23
Tần suất ĐTĐ cao trên BN COPD
* *P<0.05 vs no COPD Speaker notes The relation of COPD with the development of type 2 diabetes was assessed in a prospective cohort study, The Nurses Health Study, in which 103,614 female nurses were asked biennially from whether they had received a physician’s diagnosis of emphysaema, chronic bronchitis, asthma, and diabetes. During 8 years of follow-up, a total of 2,959 new cases of type 2 diabetes were documented of which 19 in 2,505 person-years (0.76%) occurred for nurses with COPD versus 2,940 in 726,840 (0.40%) for those with no COPD. The risk of type 2 diabetes was significantly higher for patients with COPD than those without (multivariate RR =1.8, 95% CI ). Reference Rana JS, Mittleman MA, Sheikh J, et al. Chronic obstructive pulmonary disease, asthma, and risk of type 2 diabetes in women. Diabetes Care. 2004;27: Adapted from Rana JS, et al. Diabetes Care. 2004;27: 23
 occurred for nurses with COPD versus 2,940 in 726,840 (0.40%) for those with no COPD. The risk of type 2 diabetes was significantly higher for patients with COPD than those without (multivariate RR =1.8, 95% CI ). Reference. Rana JS, Mittleman MA, Sheikh J, et al. Chronic obstructive pulmonary disease, asthma, and risk of type 2 diabetes in women. Diabetes Care. 2004;27: Adapted from Rana JS, et al. Diabetes Care. 2004;27:")
24
Tần suất cao HC chuyển hoá / COPD
47.4 P<0.05 20.6 Speaker notes Thirty-eight COPD patients in a cardiopulmonary rehabilitation program (mean FEV1 = 43 16% predicted) and 34 control participants matched for age and gender were studied to evaluate the presence of metabolic syndrome in COPD patients. The criteria for the identification of the metabolic syndrome included 3 or more of the following features: abdominal obesity (waist circumference: >102 cm in men, >88 cm in women), triglycerides level (1.69 mmol/L), high-density lipoprotein cholesterol level (<1.0 mmol/L in men, <1.3 mmol/L in women), blood pressure (130/85 mm Hg), and fasting glucose level (6.1 mmol/L). Three or more determinants of the metabolic syndrome were present in 47% of COPD patients versus 21% of control participants. Reference Marquis K, Maltais F, Duguay V, et al. The metabolic syndrome in patients with chronic obstructive pulmonary disease. J Cardiopulm Rehabil. 2005;25: * Metabolic syndrome 3 of the following: abdominal obesity, elevated triglycerides, reduced HDL-C, hypertension, hyperglycaemia Adapted from Marquis K, et al. J Cardiopulm Rehabil. 2005;25: 24
 and 34 control participants matched for age and gender were studied to evaluate the presence of metabolic syndrome in COPD patients. The criteria for the identification of the metabolic syndrome included 3 or more of the following features: abdominal obesity (waist circumference: >102 cm in men, >88 cm in women), triglycerides level (1.69 mmol/L), high-density lipoprotein cholesterol level (<1.0 mmol/L in men, <1.3 mmol/L in women), blood pressure (130/85 mm Hg), and fasting glucose level (6.1 mmol/L). Three or more determinants of the metabolic syndrome were present in 47% of COPD patients versus 21% of control participants. Reference. Marquis K, Maltais F, Duguay V, et al. The metabolic syndrome in patients with chronic obstructive pulmonary disease. J Cardiopulm Rehabil. 2005;25: * Metabolic syndrome 3 of the following: abdominal obesity, elevated triglycerides, reduced HDL-C, hypertension, hyperglycaemia. Adapted from Marquis K, et al. J Cardiopulm Rehabil. 2005;25:")
25
COPD CÓ BỆNH ĐỒNG MẮC LÀM TĂNG ĐỢT CẤP
Tim mạch: Loạn nhịp, suy tim, thuyên tắc huyết khối: TM–NMCT Hô hấp: Viêm phổi, K phế quản, OSA Tiêu hóa: Viêm loét dạ dày, GERD, hội chứng đại tràng chức năng Cơ xương: teo cơ, loãng xương Mắt: đục thủy tinh thể Chuyển hóa: Đái tháo đường, hội chứng X Máu: thiếu máu mạn đẳng sắc, đẳng bào Trầm cảm, lo âu Agusti AG, et al. Eur Respir J. 2003;21: Sevenoaks MJ, Stockley RA. Respir Res. 2006;7:70-78. Chatila et al. Proc Am Thorac Soc. 2008;5: Luppi et al. Proc Am Throrac Soc. 2008;5:

26
Tỉ lệ nhập viện cao do bệnh đồng mắc / COPD
IHD = ischaemic heart disease CHF = congestive heart failure RF = respiratory failure PVD = pulmonary vascular disease TM = thoracic malignancy — — — — — — Speaker notes This slide shows estimated prevalences of hospital discharges with selected comorbidities in patients with and without COPD derived from the National Hospital Discharge Survey from 1979 to 2001. The pink bars show patients with COPD (either as primary or secondary discharge diagnosis) and the blue bars show patients without any mention of a COPD discharge diagnosis. Results from this analysis show that discharge rates for hypertension, ischaemic heart disease (IHD), congestive heart failure (CHF), respiratory failure (RF), pulmonary vascular disease (PVD), and thoracic malignancy (TM) were all significantly higher in patients with COPD (P<0.01). References Holguin F, Folch E, Redd SC, Mannino DM. Comorbidity and mortality in COPD-related hospitalizations in the United States, 1979 to Chest. 2005;128: — — Reproduced with permission of Chest, from “Comorbidity and Mortality in COPDRelated Hospitalizations in the United States, 1979 to 2001,” Holguin F et al, Vol 128, pp , Copyright © 2005. 26
 and the blue bars show patients without any mention of a COPD discharge diagnosis. Results from this analysis show that discharge rates for hypertension, ischaemic heart disease (IHD), congestive heart failure (CHF), respiratory failure (RF), pulmonary vascular disease (PVD), and thoracic malignancy (TM) were all significantly higher in patients with COPD (P<0.01). References. Holguin F, Folch E, Redd SC, Mannino DM. Comorbidity and mortality in COPD-related hospitalizations in the United States, 1979 to Chest. 2005;128: — — Reproduced with permission of Chest, from Comorbidity and Mortality in COPDRelated Hospitalizations in the United. States, 1979 to 2001, Holguin F et al, Vol 128, pp , Copyright ©")
27
Bệnh đồng mắc và tử vong trên BN COPD Related Hospitalizations
40 COPD Non-COPD 30 Mortaliyty (%) 20 Figure 3. Estimated in-hospital mortality of hospital discharges associated with selected comorbidities in patients with and without COPD, NHDS 1979 to Bars represent the age-adjusted percentage with SE bars. Black bars show patients with COPD (either as primary or secondary discharge diagnosis). White bars show patients without any mention of a COPD discharge diagnosis. The in-hospital mortality for all listed comorbidities is different across COPD categories (p 0.01). See Comorbidity and Mortality in COPD Related Hospitalizations in the United States, 1979 to 2001* Fernando Holguin, MD; Erik Folch, MD; Stephen C. Redd, MD; and David M. Mannino, MD, FCCP Study objectives: COPD is one of the leading causes of mortality and morbidity in the United States, yet little is known about the prevalence of comorbid conditions and mortality in hospitalized patients with COPD. Design: From the National Hospital Discharge Survey, 1979 to 2001, we evaluated whether or not COPD in adults > 25 years old is associated with increased prevalence and in-hospital mortality of several comorbidities. Results: During 1979 to 2001, there were an estimated total of 47,404,700 hospital discharges (8.5% of all hospitalizations in adults > 25 years old) of patients with COPD; 37,540,374 discharges (79.2%) were made with COPD as a secondary diagnosis, and 9,864,278 discharges (20.8%) were made with COPD as the primary diagnosis. The prevalence and in-hospital mortality for pneumonia, congestive heart failure, ischemic heart disease, thoracic malignancies, and respiratory failure were larger in hospital discharges with any mention of COPD. Conclusions: In a nationally representative sample of hospitalizations, any mention of COPD in the discharge diagnosis is associated with higher hospitalization prevalence and in-hospital mortality from other comorbidities. These results highlight the fact that the burden of disease associated with COPD is likely underestimated. (CHEST 2005; 128:2005–2011) 10 Bệnh tim thiếu máu cục bộ Tăng HA Suy HH Viêm phổi Suy tim K phổi Đái tháo đường PVD Holguin et al. CHEST 2005; 128:2005
 20. Figure 3. Estimated in-hospital mortality of hospital discharges associated with selected comorbidities. in patients with and without COPD, NHDS 1979 to Bars represent the age-adjusted percentage. with SE bars. Black bars show patients with COPD (either as primary or secondary discharge. diagnosis). White bars show patients without any mention of a COPD discharge diagnosis. The. in-hospital mortality for all listed comorbidities is different across COPD categories (p 0.01). See. Comorbidity and Mortality in COPD Related Hospitalizations in the United. States, 1979 to 2001* Fernando Holguin, MD; Erik Folch, MD; Stephen C. Redd, MD; and. David M. Mannino, MD, FCCP. Study objectives: COPD is one of the leading causes of mortality and morbidity in the United. States, yet little is known about the prevalence of comorbid conditions and mortality in. hospitalized patients with COPD. Design: From the National Hospital Discharge Survey, 1979 to 2001, we evaluated whether or not. COPD in adults > 25 years old is associated with increased prevalence and in-hospital mortality. of several comorbidities. Results: During 1979 to 2001, there were an estimated total of 47,404,700 hospital discharges. (8.5% of all hospitalizations in adults > 25 years old) of patients with COPD; 37,540,374. discharges (79.2%) were made with COPD as a secondary diagnosis, and 9,864,278 discharges. (20.8%) were made with COPD as the primary diagnosis. The prevalence and in-hospital. mortality for pneumonia, congestive heart failure, ischemic heart disease, thoracic malignancies, and respiratory failure were larger in hospital discharges with any mention of COPD. Conclusions: In a nationally representative sample of hospitalizations, any mention of COPD in. the discharge diagnosis is associated with higher hospitalization prevalence and in-hospital. mortality from other comorbidities. These results highlight the fact that the burden of disease. associated with COPD is likely underestimated. (CHEST 2005; 128:2005–2011) 10. Bệnh tim thiếu máu cục bộ. Tăng HA. Suy HH. Viêm phổi. Suy tim. K phổi. Đái tháo đường. PVD. Holguin et al. CHEST 2005; 128:2005.")
28
Tử vong trên BN COPD có đái tháo đường
Đái tháo đường làm xấu đi tiên lượng của BN COPD (thời gian đến khi nhập viện lần đầu và tỷ lệ tử vong 5-năm) [1]. Theo nghiên cứu Emerging Risk Factors Collaboration [2], tỷ số nguy cơ tử vong do COPD trên BN có ĐTĐ là 1,27 so với BN không ĐTĐ. Tăng đường huyết 1mmol/L làm tăng nguy cơ tử vong 15% trên BN COPD. [3] Nguy cơ tử vong tăng (OR 1,93) và nằm viện lâu hơn là 10,3% ở BN ĐTĐ nhập viện do cơn cấp của COPD [4] Eur Respir J 2008; 32: 962–969Mannino DM, Thorn D, Swensen A, et al Seshasai SR, Kaptoge S, Thompson A, et. N Engl J Med 2011; 364: 829–841. Baker EH, Janaway CH, Philips BJ, et al. Thorax 2006; 61: 284–289 Parappil A, Depczynski B, Collett P, et. Respirology 2010; 15: 918–922
 [1]. Theo nghiên cứu Emerging Risk Factors Collaboration [2], tỷ số nguy cơ tử vong do COPD trên BN có ĐTĐ là 1,27 so với BN không ĐTĐ. Tăng đường huyết 1mmol/L làm tăng nguy cơ tử vong 15% trên BN COPD. [3] Nguy cơ tử vong tăng (OR 1,93) và nằm viện lâu hơn là 10,3% ở BN ĐTĐ nhập viện do cơn cấp của COPD [4] Eur Respir J 2008; 32: 962–969Mannino DM, Thorn D, Swensen A, et al. Seshasai SR, Kaptoge S, Thompson A, et. N Engl J Med 2011; 364: 829–841. Baker EH, Janaway CH, Philips BJ, et al. Thorax 2006; 61: 284–289. Parappil A, Depczynski B, Collett P, et. Respirology 2010; 15: 918–922.")
29
Đánh giá bệnh đồng mắc và COPD
Khảo sát COPD Bệnh đồng mắc Nếu có hút thuốc lá Speaker Notes The high prevalence of COPD and comorbidity with other serious medical conditions should prompt evaluation of COPD patients for comorbid conditions and assessment of patients who smoke with common comorbidities (e.g., cardiovascular disease, hypertension, diabetes) for COPD using spirometry. Agusti A and Jardim J, personal communication. 29
 for COPD using spirometry. Agusti A and Jardim J, personal communication. 29.")
30
VAI TRÒ THUỐC GIÃN PHẾ QUẢN ĐIỀU TRỊ COPD
TAK/COPD/12/066

32
β2-Agonists and Muscarinic Antagonists in COPD: Sites of Action

33
RecommendedFirst choice
Quản lý COPD giai đoạn ổn định, điều trị bằng thuốc Patient RecommendedFirst choice Alternative choice Other Possible Treatments A SAMA prn or SABA prn LAMA LABA SABA and SAMA Theophylline B LAMA and LABA SABA and/or SAMA C ICS + LABA LAMA and LABA or LAMA and PDE4-inh. or LABA and PDE4-inh. D and/or ICS + LABA and LAMA or ICS+LABA and PDE4-inh. or LAMA and PDE4-inh. Carbocysteine

34
Updated GOLD Recommendations: First-line Pharmacologic Therapy for Stable COPD

35
GOLD 2016 Điều trị để giảm nguy cơ kịch phát
LAMA ICS + LABA Chỉ có một nghiên cứu so sánh trực tiếp hai cách điều trị này: khó so sánh Phosphodiesterase 4 kiểu add –on cho 1 hoặc 2 Carbocysteine, SABA+SAMA và Theophylline nếu không có LABA, LAMA Wedzicha A J RRCM 2008; 177: 19-26

36
Tiotropium Respimat® giảm đáng kể nguy cơ có đợt kịch phát
50 31% Giảm nguy cơ so với placebo (P<0.0001) 40 30 Khả năng có đợt kịch phát COPD (%) Placebo SPIRIVA® Respimat® 5 µg 20 10 Results from a randomized 1-year trial of 3991 patients with chronic obstructive pulmonary disease ( ) demonstrated that tiotropium Respimat® (5 µg) delayed time to first exacerbation by 31% relative to placebo (on top of usual therapy; P<0.0001). Time to first hospital-treated exacerbation was delayed by 27% with tiotropium compared to the placebo group (P<0.005). – Tiotropium Respimat® 1-year trial including 3991 patients in 31 countries worldwide. Tiotropium Respimat® 5 µg versus placebo on top of usual therapy (other than inhaled anticholinergics). Moderate to severe patient population covered. Tiotropium Respimat® 5 µg significantly improved the coprimary study endpoint of time to first exacerbation. Reference: Bateman ED, et al. A one-year trial of tiotropium Respimat® plus usual therapy in COPD patients. Respir Med. 2010;104(10): 2 4 6 8 10 12 Duration of exposure (months) Based on time to first exacerbation data. Bateman E, et al. Respir Med. 2010;104: Study
 Khả năng có đợt kịch phát COPD (%) Placebo. SPIRIVA® Respimat® 5 µg Results from a randomized 1-year trial of 3991 patients with chronic obstructive pulmonary disease ( ) demonstrated that tiotropium Respimat® (5 µg) delayed time to first exacerbation by 31% relative to placebo (on top of usual therapy; P<0.0001). Time to first hospital-treated exacerbation was delayed by 27% with tiotropium compared to the placebo group (P<0.005) – Tiotropium Respimat® 1-year trial including 3991 patients in 31 countries worldwide. Tiotropium Respimat® 5 µg versus placebo on top of usual therapy (other than inhaled anticholinergics). Moderate to severe patient population covered. Tiotropium Respimat® 5 µg significantly improved the coprimary study endpoint of time to first exacerbation. Reference: Bateman ED, et al. A one-year trial of tiotropium Respimat® plus usual therapy in COPD patients. Respir Med. 2010;104(10): Duration of exposure (months) Based on time to first exacerbation data. Bateman E, et al. Respir Med. 2010;104: Study")
37
Tiotropium Respimat® giảm đáng kể nguy cơ có đợt kịch phát nặng
50 27% Giảm nguy cơ so với placebo (P<0.005) 40 30 Khả năng có đợt kịch phát nặng (%) 20 Placebo 10 SPIRIVA® Respimat® 5 µg 2 4 6 8 10 12 Thời gian theo dõi (tháng) Bateman E, et al. Respir Med. 2010;104: Study
 Khả năng có đợt kịch phát nặng (%) 20. Placebo. 10. SPIRIVA® Respimat® 5 µg Thời gian theo dõi (tháng) Bateman E, et al. Respir Med. 2010;104: Study")
38
NGHIÊN CỨU INSPIRE SO SÁNH ĐỐI ĐẦU ICS/LABA VỚI LAMA
1,499 BN COPD nặng (FEV1 = 39,2%) được sàng lọc 1,323 BN được phân nhóm ngẫu nhiên Salmeterol /Fluticasone FC 50/500 mcg bid (n=658) Prednisolone 30 mg Salmeterol 50 mcg bd Tiotropium 18 mcg o.d. (n=665) Thu dung trong 2 tuần; Theo dõi trong 2 năm Wedzicha JA et al. Am J Crit Care Med 2008; 177: 19–26.
 được sàng lọc. 1,323 BN được phân nhóm ngẫu nhiên. Salmeterol /Fluticasone FC 50/500 mcg bid (n=658) Prednisolone 30 mg. Salmeterol 50 mcg bd. Tiotropium 18 mcg o.d. (n=665) Thu dung trong 2 tuần; Theo dõi trong 2 năm. Wedzicha JA et al. Am J Crit Care Med 2008; 177: 19–26.")
39
KẾT QUẢ NGHIÊN CỨU INSPIRE
3.5 Salmeterol/ Fluticasone Tiotropium bromide 3 2.5 Tỷ lệ đợt cấp 2 p=0.656 p=0.039 p=0.028 1.5 1.28 1.32 0.97 0.85 1 0.82 0.69 0.5 Đợt cấp phải sử dụng dịch vụ y tế Đợt cấp phải dùng corticoid Đợt cấp phải dùng kháng sinh Wedzicha JA et al. Am J Crit Care Med 2008; 177: 19–26

40
Available and Emerging LABA and LAMA Bronchodilators for COPD

41
Effect of Indacaterol vs Blinded Tiotropium on Trough FEV1: INTENSITY

42
Single Dose of Umeclidinium/Vilanterol vs Single-Agent Components or Placebo

43
Health Status and Symptoms for Tiotropium + Olodaterol vs Monocomponents

44
Annualized Rate of Moderate or Severe Exacerbations: SPARK

45
Lung Function Improvement With Umeclidinium/Vilanterol vs Fluticasone/Salmeterol

46
Đề kháng corticoid

49
Sự khuyếch đại phản ứng viêm và kháng corticoid
Corticosteroids Thuốc lá Oxidative stress Thụ thể Glucocorticoid NF-κB Histone Acetyl hóa Inflammation Gene viêm e.g. IL-8, MMP-9 HDAC2 Barnes PJ: JCI 2008 49

50
*** Khuyếch đại viêm và kháng corticoid Kháng Steroid HDAC2 NF-κB
Thuốc lá HDAC2 expression (ratio vs histone-1) 1 2 3 Non- smokers *** Normal COPD HDAC2 Peripheral lung Ito K et al: N Engl J Med 2005 Oxidative stress ↑ phản ứng viêm Kháng Steroid NF-κB PI3K-δ Histone Acetyl hóa HDAC2 Gene viêm e.g. IL-8, MMP-9 50
 Non- smokers. *** Normal. COPD. HDAC2. Peripheral lung. Ito K et al: N Engl J Med Oxidative stress. ↑ phản ứng viêm. Kháng Steroid. NF-κB. PI3K-δ. Histone. Acetyl hóa. HDAC2. Gene viêm. e.g. IL-8, MMP")
51
ICS AND COPD PROGRESSION
TRIAL n DURATION SEVERITY Copenhagen City yr mild EUROSCOP yr mild ISOLDE yr moderate Lung Health yr moderate OUTCOME no effect 1o outcome = decline in lung function Cochrane Database Systematic Review: >13,000 COPD patients- no ↓ FEV1 decline (Yang IM et al 2007) no ↓ mortality
 no ↓ mortality.")
52
PDE4 Inhibition giữ vai trò quan trọng trong viêm
Speaker Notes Cyclic nucleotide phosphodiesterases (PDEs) are a family of enzymes that catalyse the degradation of cyclic purine (cAMP, cGMP) nucleotides to their corresponding 5’-nucleotide monophosphates.1,2 PDE4 is an enzyme which regulates the cyclic AMP (cAMP) metabolism in pro-inflammatory and immune cells.2 Activation of adenylate cyclase (AC) by cell surface receptors leads to formation of cAMP from ATP. PDE4 catalyses the breakdown of cAMP to its inactive form, AMP.1 By inhibiting the PDE4 enzyme, PDE4 inhibitors reduce the degradation of cAMP, maintaining high levels of cAMP and reducing the pro-inflammatory functions of cells.1,2 References 1. Rabe KF. Roflumilast for the treatment of chronic obstructive pulmonary disease. Expert Rev Resp Med 2010;4:543–555. 2. Hatzelmann A, Morcillo EJ, Lungarella G, et al. The preclinical pharmacology of roflumilast – A selective oral phosphodiesterase 4 inhibitor in development for chronic obstructive pulmonary disease. Pulmonary Pharm Therapeutics 2010;23:235–256. Inflammation Adapted from Rabe KF. Expert Rev Resp. Med 2010;4: 543–555. 52
 are a family of enzymes that catalyse the degradation of cyclic purine (cAMP, cGMP) nucleotides to their corresponding 5’-nucleotide monophosphates.1,2. PDE4 is an enzyme which regulates the cyclic AMP (cAMP) metabolism in pro-inflammatory and immune cells.2. Activation of adenylate cyclase (AC) by cell surface receptors leads to formation of cAMP from ATP. PDE4 catalyses the breakdown of cAMP to its inactive form, AMP.1. By inhibiting the PDE4 enzyme, PDE4 inhibitors reduce the degradation of cAMP, maintaining high levels of cAMP and reducing the pro-inflammatory functions of cells.1,2. References. 1. Rabe KF. Roflumilast for the treatment of chronic obstructive pulmonary disease. Expert Rev Resp Med 2010;4:543– Hatzelmann A, Morcillo EJ, Lungarella G, et al. The preclinical pharmacology of roflumilast – A selective oral phosphodiesterase 4 inhibitor in development for chronic obstructive pulmonary disease. Pulmonary Pharm Therapeutics 2010;23:235–256. Inflammation. Adapted from Rabe KF. Expert Rev Resp. Med 2010;4: 543–")
53
PDE4 Inhibitors tác động lên tất cả TB trong COPD
Airway smooth muscle cells CD8+ T-cell Epithelial cells Capillary Macrophage PDE4 Inhibitor NANC nerves Sensory nerves Speaker Notes In contrast to asthma, the key inflammatory cells involved in COPD are CD8+ T-cells, neutrophils and macrophages, all of which are targets for PDE4 inhibitors.1,2 PDE4 inhibitors also target structural cells, in which PDE4 is present, for example attenuating airway smooth muscle proliferation and modulating neuronal control of pulmonary function via NANC and sensory nerves.1 In contrast to asthma, airway inflammation in COPD is characterised by a neutrophilic inflammation with increased numbers of macrophages and CD8+ T-cells. These cells release the reactive oxygen species, chemokines (e.g. IL-8), cytokines (e.g., TNF-) and proteases (e.g., neutrophil elastase and matrix metalloproteinase) that are instrumental in producing a chronic inflammatory state. The ongoing inflammatory processes lead to enlargement of the alveolar spaces, destruction of the lung parenchyma, loss of elasticity and small airways obstruction. Airway hyperresponsiveness is not a feature of COPD. Epithelial metaplasia and mucus hypersecretion are prominent features of COPD.2 Unlike the treatment of asthma, where corticosteroids suppress eosinophilic inflammation, it is not clear whether corticosteroids have significant anti-inflammatory effects in COPD. There are minimal changes in neutrophilic inflammation and no reductions in inflammatory mediators and proteases.2 References 1. Barnette MS, Underwood D. New PDE inhibitors as therapeutics for the treatment of chronic lung disease. Curr Opin Pulm Med 2000; 6: 164–169. 2. Barnes PJ. Mechanisms of COPD. Differences from asthma. Chest 2000; 117 (Suppl 2): 10S–14S. Neutrophil Fibroblast NANC=Nonadrenergic and Noncholinergic Adapted from Barnette MS, et al. Curr Opin Pulm Med 2000; 6: ; and Hatzelmann A, et al. Pulmonary Pharmacol & Ther. 2010;23: 53
, cytokines (e.g., TNF-) and proteases (e.g., neutrophil elastase and matrix metalloproteinase) that are instrumental in producing a chronic inflammatory state. The ongoing inflammatory processes lead to enlargement of the alveolar spaces, destruction of the lung parenchyma, loss of elasticity and small airways obstruction. Airway hyperresponsiveness is not a feature of COPD. Epithelial metaplasia and mucus hypersecretion are prominent features of COPD.2. Unlike the treatment of asthma, where corticosteroids suppress eosinophilic inflammation, it is not clear whether corticosteroids have significant anti-inflammatory effects in COPD. There are minimal changes in neutrophilic inflammation and no reductions in inflammatory mediators and proteases.2. References. 1. Barnette MS, Underwood D. New PDE inhibitors as therapeutics for the treatment of chronic lung disease. Curr Opin Pulm Med 2000; 6: 164– Barnes PJ. Mechanisms of COPD. Differences from asthma. Chest 2000; 117 (Suppl 2): 10S–14S. Neutrophil. Fibroblast. NANC=Nonadrenergic and Noncholinergic. Adapted from Barnette MS, et al. Curr Opin Pulm Med 2000; 6: ; and Hatzelmann A, et al. Pulmonary Pharmacol & Ther. 2010;23:")
54
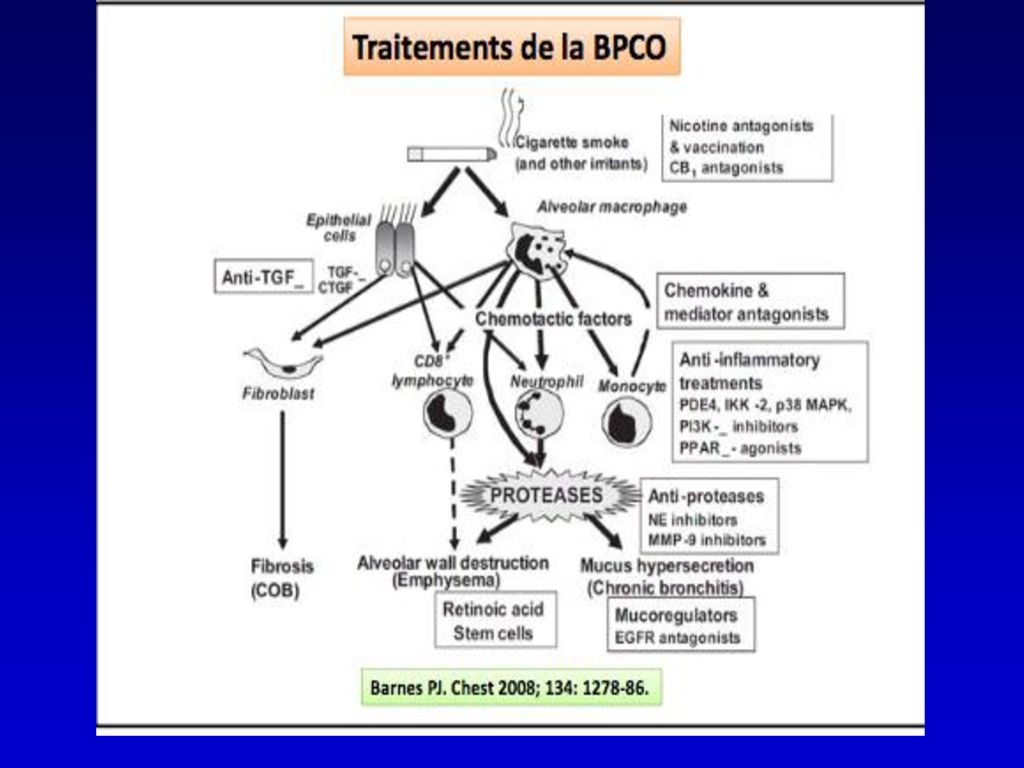
is corticosteroid-resistant
COPD INFLAMMATION Cigarette smoke (and other inhaled irritants) Epithelial cells Macrophage Neutrophil Tc1 cell Monocyte Th1 cell CXCL1 CXCL8 CXCR3 CXCR2 CCR2 CCL2 CXCL9,10,11 TGF-β Fibrosis (Small airways) Fibroblast COPD inflammation is corticosteroid-resistant PROTEASES Neutrophil elastase MMP-9 Alveolar wall destruction (Emphysema) Mucus hypersecretion Barnes PJ: Nat Rev Immunol 2008.
 Epithelial cells. Macrophage. Neutrophil. Tc1 cell. Monocyte. Th1 cell. CXCL1. CXCL8. CXCR3. CXCR2. CCR2. CCL2. CXCL9,10,11. TGF-β. Fibrosis. (Small airways) Fibroblast. COPD inflammation. is corticosteroid-resistant. PROTEASES. Neutrophil elastase. MMP-9. Alveolar wall destruction. (Emphysema) Mucus hypersecretion. Barnes PJ: Nat Rev Immunol")
55
Kết luận COPD: gánh nặng lớn, tử vong cao tần suất đang gia tăng
Tiotropium cải thiện triệu chứng, chức năng hô hấp, chất lượng cuộc sống. Khả năng gắng sức, làm giảm đợt kịch phát và tử vong Hiệu quả của Tiotropium càng rõ ở BN COPD ở giai đoạn sớm GOLD 2. Tiotropium + LABA tăng thêm hiệu quả giãn phế quản.

57
XIN CÁM ƠN QUÍ ĐỒNG NGHIỆP

Các bản thuyết trình tương tự








>")


 tại Nhật Bản HORII Satoko, Ph.D, RN, PHN Cố vấn trưởng dự án “Tăng cường hệ thống.>")
>")







